
Delayed-type hypersensitivity is a T-cell mediated immune response occurring 24-72 hours post-antigen exposure. Antigen-presenting cells sensitize T-cells, which upon re-exposure release cytokines, activating local endothelial cells and macrophages, resulting in inflammation and swelling.
Oxazolone-induced delayed-type hypersensitivity (DTH) mice model is a valuable tool for exploring the mechanisms and pathophysiology of DTH-associated chronic inflammatory diseases. This mice model is significant in assessing the potential therapeutic candidates against chronic inflammatory diseases. Thus, bridging the gap between preclinical studies and potential clinical applications against inflammatory conditions.
At Aragen, our team validated the oxazolone-induced DTH mice model, simulating a controlled environment for comprehending the mechanisms underlying T-cell-mediated DTH response and investigating the pathophysiology of chronic inflammatory diseases like atopic dermatitis (AD). This model is useful for evaluating the efficacy of potential anti-inflammatory and immunosuppressive agents against DTH-associated inflammatory skin diseases.
This case study details Aragen’s capability to establish the oxazolone-induced DTH mice model for simulating atopic dermatitis (a chronic relapsing inflammatory skin disease) pathophysiology and assessing the therapeutic potential of clobetasol-an anti-inflammatory corticosteroid in modulating the resultant chronic DTH response in female BALB/c mice (18-22 g). Animals were assigned randomly to three groups (n = 8-10/group): normal control, oxazolone/vehicle and oxazolone/ clobetasol groups.
To begin, the basal ear thickness was measured and then on day zero, 0.5% oxazolone was applied to the exposed abdominal area-sensitizing the immune system. On day 5, 10, 15 and 20, the animals were challenged by applying oxazolone to the ear, eliciting the DTH reaction. About half an hour before the challenge, clobetasol (20mg/mouse) was applied topically to the ear of the groups (oxazolone/vehicle and oxazolone/ clobetasol) to evaluate its therapeutic effect.
After the final challenge (on day 21), the ears were collected and processed for histopathological examination (hematoxylin & eosin staining) and a histopathology score was assigned by evaluating the magnitude of the AD-like skin symptoms. The changes in spleen weight of test groups were compared to control group for assessing the extent of elicited systemic immune response.
The oxazolone-induced mice model is mostly used as a DTH model. After oxazolone (hapten) application, acute phase of DTH appears as an initial increase in ear thickness due to onset of inflammation. Later, with multiple oxazolone challenges over an extended time (days), the extent of ear thickness might stabilize (normal control) or continue to increase depending on the treatment given (oxazolone/vehicle and oxazolone/clobetasol) (Figure 1). A further increment in ear thickness indicates chronic DTH that involves persistent inflammation and immune cell infiltration. This shift from a typical acute DTH response to a chronic inflammatory response (Figure 1) is characteristic of AD.

Figure 1: Delayed-type hypersensitivity (DTH) response post oxazolone application in normal control, oxazolone/ vehicle and oxazolone/ clobetasol groups.
Oxazolone application induces AD-like skin symptoms in mice that manifest as histopathological changes such as acanthosis (thickening of the epidermis), parakeratosis (excessive keratin formation), hyperkeratosis (skin thickening due to excessive keratin deposition), and continued inflammation. Treatment with clobetasol attenuates these AD-like skin symptoms as depicted from the figure 2A (H & E staining) and figure 2B (ear histopathology score). Clobetasol is a potent topical steroid exhibiting anti-inflammatory, immunosuppressive, vasoconstrictive, and cellular effects that bestow it therapeutic efficacy against dermatological conditions like eczema, dermatitis, psoriasis, etc.
Ear Histopathology (H & E staining)

Ear Histopathology Score
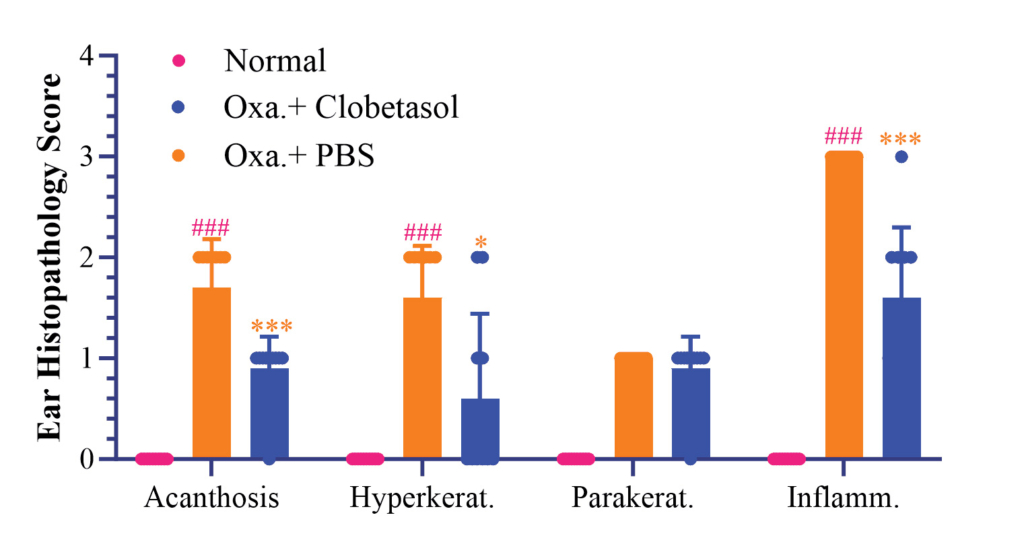
Figure 2: Ear histopathology score (A) and hematoxylin & eosin (H & E) staining (B) for normal control, oxazolone/vehicle and oxazolone/ clobetasol groups.
Spleen is the main site for the production and storage of leukocytes, including the T-cells that mediate DTH reactions. The measurement of spleen weight provides an indirect estimation of systemic immune activation. An increase in spleen weight compared to control group indicates an enhanced immune response as observed for oxazolone/vehicle group. Whereas clobetasol application caused reduced spleen weight as seen in oxazolone/clobetasol group (Figure 3), demonstrating its immunosuppressive effect. Conclusively, the results of this study corroborated with previous findings, confirming our proficiency in the establishment of a successful oxazolone-induced DTH mice model.

Figure 3: Changes in spleen weight in the control and the treatment groups (oxazolone/vehicle and oxazolone/
clobetasol groups).
At Aragen, we are committed to facilitate our client’s IND-enabling in vivo studies. Our comprehensive services include:
